
Why is the incidence of unwanted effects from statins so low in medical trials whereas showing to be so excessive in the true world?
“There may be now overwhelming proof to help lowering LDL-C (low-density lipoprotein ldl cholesterol)”—so-called unhealthy ldl cholesterol—to cut back atherosclerotic heart problems (CVD),” the primary killer of women and men. So, why is adherence to cholesterol-lowering statin drug remedy such “a serious problem worldwide”? Researchers discovered “that almost all of research reported that a minimum of 40%, and as a lot as 80%, of sufferers didn’t comply totally with statin therapy suggestions.” Three-quarters of sufferers could flat out cease taking them, and nearly 90 % could discontinue therapy altogether.
When requested why they stopped taking the tablets, most “former statin customers or discontinuers…cited muscle ache, a facet impact, as the first cause…” “SAMSs”—statin-associated muscle signs—“are by far probably the most prevalent and necessary adversarial occasion, with as much as 72% of all statin adversarial occasions being muscle-related.” Taking coenzyme Q10 dietary supplements as a therapy for statin-associated muscle signs was a good suggestion in concept, however they don’t seem to assist. Usually, side-effect signs go away whenever you cease the drug however can typically linger for a 12 months or extra. There is “rising proof that statin intolerance is predominantly psychosocial, not pharmacological.” Actually? It could be principally simply in folks’s heads?
“Statins have developed a foul fame with the general public, a phenomenon pushed largely by proliferation on the Web of weird and unscientific however seemingly persuasive criticism of those medicine.” “Does Googling result in statin intolerance?” However folks have stopped taking statins for many years earlier than there even was an Web. What sorts of information have docs instructed that sufferers are falsely “misattribut[ing] regular aches and pains to be statin unwanted effects”?
Effectively, for those who take individuals who declare to have statin-related muscle ache and randomize them forwards and backwards between statins and an identical-looking placebo in three-week blocks, they’ll’t inform whether or not they’re getting the true drug or the sugar tablet. The issue with that examine, although, is that it might take months not solely to develop statin-induced muscle ache, however months earlier than it goes away, so no surprise three weeks on and three weeks off will not be lengthy sufficient for the members to discern which is which.
Nonetheless, these knowledge are extra convincing: Ten thousand folks had been randomized to a statin or a sugar tablet for just a few years, however so many extra folks had been dying within the sugar tablet group that the examine needed to be stopped prematurely. So then everybody was provided the statin, and the researchers famous that there was “no extra of stories of muscle-related AEs” (adversarial results) amongst sufferers assigned to the statin over these assigned to the placebo. However when the placebo section was over and the folks knew they had been on a statin, they went on to report extra muscle unwanted effects than those that knew they weren’t taking the statin. “These analyses illustrate the so-called nocebo impact,” which is akin to the other of the placebo impact.
Placebo results are constructive penalties falsely attributed to a therapy, whereas nocebo results are unfavorable penalties falsely attributed to a therapy, as was evidently seen right here. There was an extra fee of muscle-related adversarial results reported solely when sufferers and their docs had been conscious that statin remedy was getting used, and never when its use was hid. The researchers hope “these outcomes will assist guarantee each physicians and sufferers that almost all AEs related to statins are usually not causally associated to make use of of the drug and may assist counter…exaggerated claims about statin-related unwanted effects.”
These are the sorts of outcomes from “placebo-controlled randomised trials [that] have proven definitively that just about all the symptomatic adversarial occasions which might be attributed to statin remedy in routine apply are usually not really attributable to it (ie, they signify misattribution.)” Now, “just a few sufferers will consider that their SAMS are of psychogenic origin” and simply of their head, however their denial could have “lethal penalties.” Certainly, “discontinuing statin therapy could also be a life-threatening mistake.”
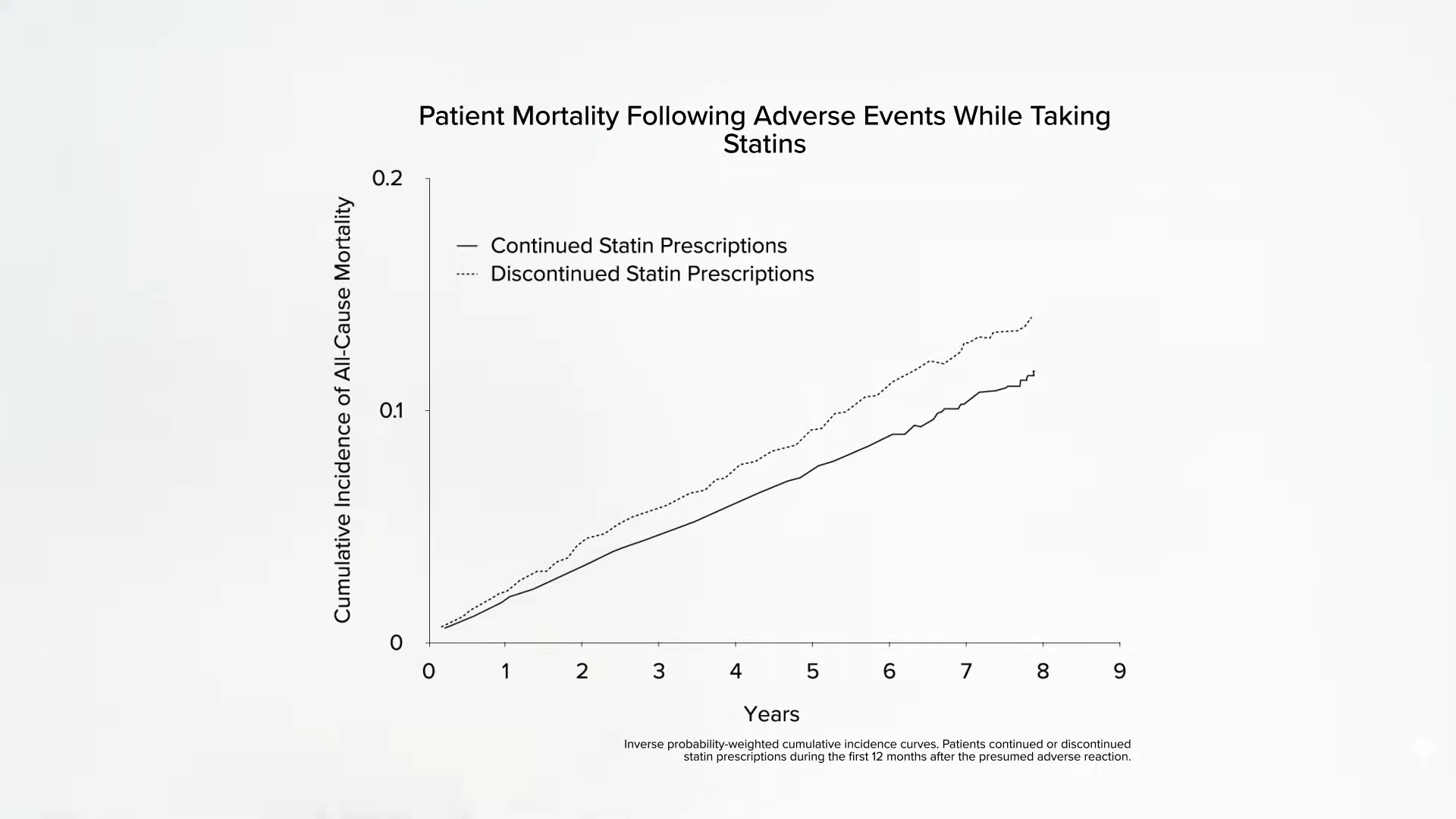
Beneath and at 4:46 in my video How Widespread Are Muscle Facet Results from Statins?, you possibly can see the mortality of those that stopped their statins after having a doable adversarial response in comparison with those that caught with them. This interprets into about “1 extra dying for each 83 sufferers who discontinued therapy” inside a four-year interval. So, when there are media stories about statin unwanted effects and folks cease taking them, this may “lead to 1000’s of deadly and disabling coronary heart assaults and strokes, which might in any other case have been prevented. Seldom within the historical past of recent therapeutics have the substantial confirmed advantages of a therapy been compromised to such an extent by severe misrepresentations of the proof for its security.” However is it a misrepresentation to recommend “that statin remedy causes side-effects in as much as one fifth of sufferers”? That is what’s seen in medical apply; between 10 to 25 % of sufferers positioned on statins complain of muscle issues. Nonetheless, as a result of we don’t see wherever close to these sorts of numbers in managed trials, sufferers are accused of being confused. Why is the incidence of unwanted effects from statins so low in medical trials whereas showing to be so excessive in the true world?
Take this meta-analysis of medical trials, for instance: It discovered muscle issues not in 1 in 5 sufferers, however only one in 2,000. Ought to everybody over a sure age be on statins? Not surprisingly, each a kind of trials was funded by statin producers themselves. So, for instance, “how may the statin RCTs [randomized controlled trials] miss detecting gentle statin-related muscle adversarial unwanted effects similar to myalgia [muscle pain]? By not asking. A evaluation of 44 statin RCTs reveals that only one instantly requested about muscle-related adversarial results.” So, are the overwhelming majority of unwanted effects simply being missed in all these trials, or are the overwhelming majority of unwanted effects seen in medical apply only a figment of sufferers’ creativeness? The underside line is we don’t know, however there may be definitely an pressing must determine it out.



{kind=link}